How to Increase Natural Testosterone Levels

In the private medical sector, particularly in some parts of the world, we feel that too many patients are put onto Testosterone Replacement Therapy (TRT) unnecessarily, and that due diligence is not always shown before signing someone up to what is a lifelong therapy. Disappointingly, many TRT providers are preying on men at their most vulnerable and using TRT as a ‘cash-cow’. To use a familiar expression:
“Congratulations! You qualify for TRT. Welcome to a new, BETTER you!”
In contrast, our ethos has always been one of prevention, where we will always strive to act in your best interests. The decision to start TRT should always be a considered one, balancing the benefits of treatment against the potential risks, and weighing up the long term commitment of both your time and financial resources. To quote the original ancient Hippocratic oath, “Primum non nocere”, which (for those illiterate in Latin, like myself) translates to, “First do no harm”. TRT is available to treat hypogonadism, but ONLY when there is clear indication that treatment is needed. It could otherwise be harmful, in one capacity or another, for you to take TRT when it’s NOT necessary.
Exogenous testosterone suppresses your body’s own natural production of testosterone, and so if you ever decide to stop therapy, the continued use of TRT will decrease your chance of being able to recover year on year, particularly if not using Human Chorionic Gonadotrophin (HCG). This is why, when the decision is made to commence a patient on treatment, we subscribe to the mantra of maintaining function whilst optimising your male androgen levels, with the use of testosterone and HCG. The use of HCG is discussed further in Dr Stevens’ blog ‘The Benefits Of HCG With TRT’. Disappointingly, HCG is not routinely offered in private practice, nor is it considered necessary within the NHS.
If there isn’t a clear indication that TRT is the only solution for you, then looking at natural methods to increase your testosterone levels first is always advisable, especially given that many cases of low testosterone are caused by poor lifestyle habits. Altering these habits will contribute to innumerable positive benefits across your life, in both mental and physical well being and health. Understandably, in extreme circumstances it becomes near impossible to take action and do anything but start TRT. But, for the rest of those reading who don’t fit into the categories where it is absolutely unavoidable, I want to talk to you about the ways we can try to naturally get increase our testosterone, find an optimal balance and avoid any unnecessary treatment. Lets start by learning about what reversible causes can cause a reduction in testosterone.
Revisiting The HPGA & More – Balls, Brain, Fat, Liver & The Average Joe
The control of the Hypothalamus pituitary gonadal axis in men is more complex than simple diagrams make it out to be. They often miss out our T à E2 conversion steps, inhibin production and so on. As a recap at the most basic level, the following happens (I’ve highlighted the most important bits – feel free to read these parts only):
- The hypothalamus, stimulated by the medial preoptic nucleus, secretes Gonadotropin-releasing hormone (GnRH) into the hypophysial portal bloodstream at the medial eminence, which is carried to the pituitary gland. This is pulsatile in nature, ie. it happens at regular intervals.
- GnRH stimulates the synthesis and secretion of follicle-stimulating hormone (FSH) and luteinising hormone (LH) in the pituitary gland. A low frequency GnRH pulse ensures FSH release, whereas a high-frequency pulse stimulates LH pulses 1.
- LH stimulates the Leydig cells of the testes to produce Testosterone. FSH acts synergistically here. Intratesticular oestradiol is also produced, as is inhibin, which negatively feeds back to inhibit to production of FSH in the pituitary gland.
- Both the liver and adipose tissue act as major sites for the conversion of testosterone to oestradiol via the aromatase enzyme.
- Oestradiol and Testosterone both feedback negatively to inhibit the production of GnRH at the Hypothalamus, as well as LH and FSH production and secretion at the pituitary gland.
As the output of T and E2 drop due to inhibition, an increase in GnRh and subsequent LH and FSH can occur, in normal healthy individuals. I’ve created a diagram to represent these steps below, in Figure 1.
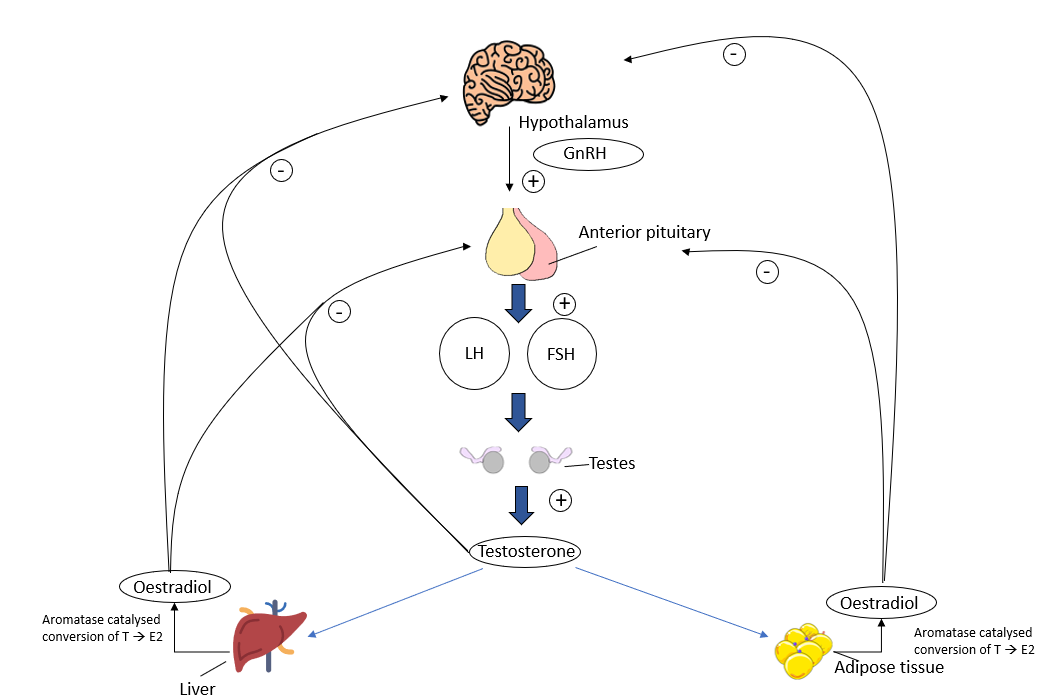
Figure 1 – Basic diagram of the HPTA and its negative feedback loop (click for full-size image)
This is still an oversimplified explanation of the process, and is mostly only true for the average fit and healthy Joe. Things become much more complex in diseased and malnutritional states due to a multitude of biomedical reasons.
What Could Disrupt The HPTA To Cause A Reversible Lowering Of Testosterone?
As mentioned, many things can cause the lowering of Testosterone. To be clear, I will be talking primarily about things that are within our control.
You may think that one such example is short term anabolic-androgenic steroids (AAS) use, where AAS induce hypogonadotropic hypogonadism 2. But let’s clarify that, in some individuals, the negative effects of AAS persist for long periods of time. Not every patient will escape the burdens of irreversible AAS induced hypogonadism. We know this both clinically (first hand) and within the reported literature 3,4. So, AAS are NOT included in this list. Does it mean that if you’ve taken AAS, you should automatically be put onto TRT afterwards? No, TRT is there for these groups of people, but only where recovery is NOT possible.
So, what affects natural Testosterone adversely? Here is a list of things that we can control or reverse:
- Inadequate Sleep
- Malnutrition
- Excess Weight
- Underweight
- Sedentary Behaviour
- Chronic High Stress
- Alcohol
- Reversible Non-Communicable Diseases – ie. Type 2 Diabetes Mellitus
- Endocrine Disruptors (EDCs)
Let’s go through these…
Inadequate Sleep
If you’ve already read my blog on the Endocrine System & Sleep you’d know why a lack of sleep is bad. Not merely because it does indeed lower Testosterone 5, but also because of the various other negative effects it has on us.
In a healthy sleep routine, we would see a peak in pulsatile LH secretion during sleep, requiring a minimum of at least 3 hours of sleep. But, 7 to 8 hours is much more ideal. Let’s have a reminder of what sleep deprivation does to us with the below summarised table 6,7.
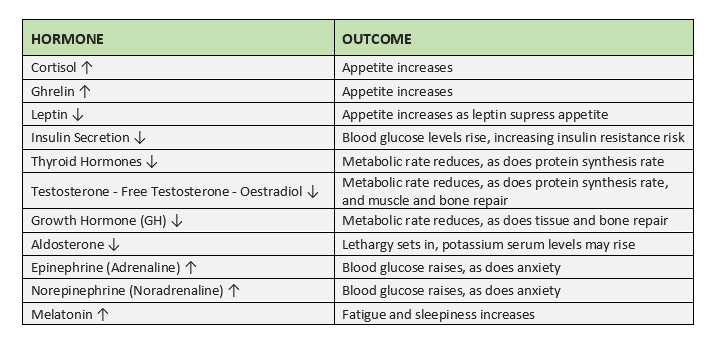
Table 1 – Effects of sleep deprivation on hormones and the relative outcomes (click for full-size image)
Sleep apnoea is testament to the devastating effects that poor sleep quality or inadequate sleep duration can do to our natural testosterone levels, among many other systems in our bodies.
Malnutrition
Eating too little of the essential things we need, or excess calories to the point we become insulin resistant and overweight, will indeed negatively affect our testosterone levels. They’ll also affect many other things in our body.
To quote one study 8:
“The total T-related dietary pattern (a high consumption of bread and pastries, dairy products, and desserts, eating out, and a low intake of homemade foods, noodles, and dark green vegetables) independently predicted hypogonadism (odds ratio: 5.72; 95% confidence interval: 1.11‒29.51, p < 0.05) for those with the highest dietary pattern scores (Q4) compared to those with the lowest (Q1).”
In plain English, this means that inadequate whole foods which contain vitamins and minerals that are essential to our well being and health, concurrent with a caloric excess, will enormously increase the risk of hypogonadism. The common western style diet, which is high in processed foods, carbohydrates, low in essential fats, low in whole foods, low in vitamins and minerals, vegetables, fruit, and high in saturated and trans, is not conducive to improving Testosterone levels 9,10. You may be thinking, “What if it fits my macros?” – the likelihood is if you follow this, and do indeed get enough macro and micronutrients, then you’re probably also exercising too. A high calorie and high carbohydrate diet is fine, if you exercise and are therefore able to control your blood sugar and weight. To the average person, this is absolutely not the case.
On the topic of caloric intake, this largely depends on how it ultimately affects your weight, and if you are indeed exercising. A resistance trained male eating in a moderate caloric excess may in fact see slight increases in testosterone, which are more significant if they’ve been chronically dieting for some time. Contrastingly, long term calorie restriction, particularly in the extremes, will also lead to lowered testosterone. Even if getting adequate micronutrients 11.
Excess Weight
Malnutrition heavily ties in with body composition. Being obese or overweight is incredibly bad for natural testosterone levels and I detail this to great depths with the scientific evidence in my ‘Me & My Fat – The Role of Fat on Your Hormonal Health’ blog. Excess fat will lend to an increase in oestradiol, which ultimately lowers our testosterone, as evident from Figure 1. Likewise, numerous metabolic changes occur which also decrease total testosterone, such as an increase in leptin production (altering Leydig cell function), increased adipokines production (leading to an increased pro-inflammatory state), worsened insulin sensitivity, increased risk of sleep apnoea and much more. All of this leads to a much greater risk of lowered natural testosterone levels.
Underweight
As expected, being significantly underweight also causes large reductions in testosterone, which of course is highly related to the malnutrition state required to be underweight. Sadly, hypogonadotropic hypogonadism can often persist even after weight restoration – it takes time to resolve and reverse 12.
Sedentary Behaviour
Exercise is well known to contribute to normal testosterone levels, in addition to better overall physical and mental health 13–15. Thus, it’s no surprise that sedentary behaviour lowers testosterone 16. This is due to the various metabolic and other adaptations induced by exercising, which is a lengthy enough topic that an explanation of it deserves its own article.
Chronic High Stress
High stress levels will indeed reduce testosterone levels, due to the inverse relationship between the primary stress hormone cortisol and testosterone. This is also detailed to great lengths in my ‘Stress & Testosterone‘ blog. To reiterate, we see reductions in natural testosterone in those with chronic high stress levels, not so much acutely high levels of stress seen in sudden stressful situations such as a fight, exam, and so on. In fact, we have observed significant increases in testosterone in acute stress environments, such as just prior to an exam 17.
Alcohol
Alcohol is unfortunately just bad all round for guys when it comes to testosterone. I also detailed this with my ‘Alcohol, Sex Hormones & Cardiometabolic Health‘ blog. I mentioned in this blog that you should simply drink responsibly and not excessively; living life happily is still important, and if it means you want to drink within moderation, then go for it.
Reversible Non Communicable Diseases
By this I largely refer to metabolic syndrome and Type 2 Diabetes Mellitus (T2DM). Both are well known to be linked with hypogonadism, though it often raises the chicken and egg question that I so frequently come back to. In these instances though, all the associated outcomes of T2DM and metabolic syndrome lead to an environment that’s ideal for hypogonadism. That includes excess adipose tissue, increased sedentary behaviour, and insulin and leptin resistance.
Can you reverse T2DM? Indeed, you can. This may involve use of bariatric surgery, low-calorie diets, or carbohydrate restriction 18. For many cases, the cause is often lifestyle related; excess chronic alcohol consumption, excess calories and a sedentary lifestyle. Of course, genetic predispositions exist, especially for some ethnicities. I am included in this category, being mixed ethnicity with my maternal line being South Asian in origin. Keeping my blood sugar in check during the festive periods can be a nightmare! There are additional risk factors too, including gut metagenome, ie. the bacteria you have in your gut, which can be altered by the foods you eat and any medications that you may take. Vitamin K and Vitamin D deficiency also increases the risk of T2DM, as does smoking and obstructive sleep apnoea 19. Thus, getting enough Vitamin K and Vitamin D, exercising more, eating more green vegetables and fibre, reduced red meat consumption but increased fatty fish, soy, dairy and dairy products, drinking less, eating less calories, and even having probiotic milks, such as Yakult, will help protect you against T2DM 22,23.
EDCs
Endocrine disruptors, not electronic daisy carnival (a bad joke I’ve made before). I’ve also extensively written about this topic in my blog on Endocrine Disruptors & The HPG Axis. For the most part, many EDCs are unavoidable and the scale of effects they have on the endocrine system are difficult to identify in the real world. So, what was the verdict? Avoid BPAs, avoid being around wildfires, and don’t purposely go about trying to inhale as much smoke as possible from fires either.
What Can I Do To Increase My Natural Testosterone Levels?
There are several things you should be doing to help ensure you have the best environment to improve natural testosterone. I’ve listed them below:
Sleep Enough
And, if doing shift work, plan your sleep as much as you can. Always aim for a minimum number of hours to make yourself feel refreshed, generally 7-8 hours is ideal for most people.
If You Have Sleep Apnoea & Are Overweight…
Try a calorie restriction diet and see if a large amount of weight loss helps to improve it. If it persists, or you aren’t overweight, get it investigated! At The Men’s Health Clinic we offer sleep studies, CPAP therapy and full sleep support services through our professional partnership with Phillips. Check out our Sleep Health page for more information.
Eat Right
Eating right is crucial to all aspects of your health, not just to increase your testosterone:
- You need to be eating green leafy vegetables, more fibre, and preferably reduce and swap more of your red meat consumption for white meat, eggs, fish (especially fatty fish), and plant proteins.
- Try to eat foods such as nuts, oats, milk, cheese, broccoli, green beans, salmon, chicken and legumes. Do try making it as enjoyable as possible so that you can stick to eating healthily.
- Eat whole non-processed foods, avoiding trans fats like the plague. Eat more poly unsaturated fatty acids, often found in fatty fish.
- Eat enough calories, but not an excess of them (ie. enough to gain weight) or too little (ie. anorexia or attempting to reach extremely low (under 7%) body fat percentages.
Check Your Micronutrient Levels
Supplement with Vitamin D if you need to. Obviously, this depends on how much sunlight you get. If you get adequate exposure or are in the sun all day (do wear sunscreen if you are in the sun all day i.e. driving a lorry for long periods of time), you won’t need to supplement as much. How much this would be varies person to person and also depends on how dark your skin is. The darker, the more vitamin D you may need. I personally do fine with 5000iu a day to keep above 30 ng/mL of 25-hydroxy-vitamin D, one study demonstrated that in Saudi Arbian men and women, 2000 iu/day was NOT enough to keep above this 20. So, get your blood test results for vitamin D, dose up, and reassess! As mentioned, your skin tone will play a role here in how much Vitamin D you may or may not need, concurrent with how much sunlight exposure you get.
Likewise, also consider supplementing Zinc at 25-100mg per day, to help with potentially reducing liver specific aromatisation. But, do consider maintaining adequate copper intake to balance your zinc/copper ratio, as copper is important and zinc competes with copper for binding sites. How much is enough? One study suggested 80mg of elemental zinc (100mg zinc oxide) with 2mg of copper for preventing age related macular degeneration in a safe manner, so this is likely a fine dose to supplement 21.
You can also supplement a multivitamin but be warned that the fat-soluble vitamins in it can build up, sometimes to toxic levels. Therefore, proceed with caution and avoid foods high in fat soluble vitamins that can cause toxicity, ie. Liver (Vitamin A). The same level of caution should be approached with B vitamin complexes. Vegetarians take note – you need to supplement B vitamin complexes and you may well need to source additional iron – check your blood tests. Irrespective, strive to eat foods that are high in the specific micronutrients you need, as supplementation is merely that; to supplement what should be an already whole-food rich and healthy diet.
Eat Less Carbohydrates
I said less, you don’t need to drop them entirely, and eat more protein. If you are overweight, use a moderate deficit to lose fat, not an excessive one. You can safely lose fat, with far less issues, at a 20% calorie deficit.
Try Probiotics!
If You Smoke…
Try to get onto programmes to get off it. Smoking is bad to health regardless.
Have A Healthy Body Fat % & Exercise
Ensure that you’re at a healthy body fat percentage (anywhere between 10-17%), and exercise!
- Do resistance training/strength training routine, concurrent with plenty of cardiovascular exercise such as running and cycling.
- Do cardiovascular exercise daily. If you’re too heavy to run comfortably and can’t cycle, go walking plenty. Get a step counter and aim for a minimum of 10k steps per day.
- No gym? No problem. Get resistance bands, do body weighted routines, think outside the box.
- Have an office job? Try standing up more often at your desk, take frequent mini breaks and get a little walk about if you can. Sitting down for extended hours is not only bad for your health and back, but it’s also bad for your mental health.
Destress
Try meditation and find activities which help you to destress.
- Have excessive work stress that’s turned chronic? Try talking to your manager. There are procedures in place to ensure your work safety so if your manager doesn’t want to help, seek advice elsewhere such as at a work union.
- Take a break or a holiday.
- Stress elsewhere? Seek professional help, don’t let your mental health deteriorate.
Drink In Moderation
Drink two units a day at most. Don’t binge drink. Alcohol can help you to relax and destress, but it can become a problem too, so keep that in mind.
Have T2DM?
Try seeing if you can reverse it with diet and exercise.
Avoid BPAs
…and inhaling smoke for prolonged periods of times.
Of course, even after months or potentially a year of following all of this fully and properly, you may still find you haven’t improved. This is where medical investigation is absolutely warranted as there may be bigger problems that need resolving. If you require TRT and we agree with that assessment, we would be more than happy to help you. We put both physical and mental health first and foremost above everything else, ergo we will only treat you if you truly need treatment. Remember, TRT is a lifelong commitment.
Conclusions
As highlighted in this blog. there are multiple ways of trying to improve your own natural testosterone levels. At The Men’s Health Clinic, we care about your personal health and well being above all else. We will therefore always assess whether its possible for you to increase your own natural testosterone first, before intervening. TRT is a lifelong commitment that requires dialling in and adjustment, and so is not something to be take lightly. Unless you’ve been diagnosed with a clear cause of hypogonadism, where treatment is inevitable, we recommend that you start by taking steps to naturally improve your testosterone and sex steroid hormone levels, before considering treatment. Regardless, we will be here to help you along your journey to better health, whether by natural means, or via treatment.
References
- Lüking Jayes FC, Britt JH, Esbenshade KL. Role of Gonadotropin-Releasing Hormone Pulse Frequency in Differential Regulation of Gonadotropins in the Gilt. Biol Reprod. 1997;56(4):1012-1019. doi:10.1095/biolreprod56.4.1012
- El Osta R, Almont T, Diligent C, Hubert N, Eschwège P, Hubert J. Anabolic steroids abuse and male infertility. Basic Clin Androl. 2016;26(1). doi:10.1186/s12610-016-0029-4
- Boregowda K, Joels L, Stephens JW, Price DE. Persistent primary hypogonadism associated with anabolic steroid abuse. Fertil Steril. 2011;96(1). doi:10.1016/j.fertnstert.2011.04.029
- Kanayama G, Hudson JI, Deluca J, et al. Prolonged hypogonadism in males following withdrawal from anabolic-androgenic steroids: An under-recognized problem. Addiction. 2015;110(5):823-831. doi:10.1111/add.12850
- Leproult R, Van Cauter E. Effect of 1 week of sleep restriction on testosterone levels in young healthy men. JAMA – J Am Med Assoc. 2011;305(21):2173-2174. doi:10.1001/jama.2011.710
- Joo EY, Yoon CW, Koo DL, Kim D, Hong SB. Adverse effects of 24 hours of sleep deprivation on cognition and stress hormones. J Clin Neurol. 2012;8(2):146-150. doi:10.3988/jcn.2012.8.2.146
- Tae Won Kim J-HJ, Hong S-C. The Impact of Sleep and Circadian Disturbance on Hormones and Metabolism. International Journal of Endocrinology. doi:10.1155/2015/591729
- Hu TY, Chen YC, Lin P, et al. Testosterone-associated dietary pattern predicts low testosterone levels and hypogonadism. Nutrients. 2018;10(11). doi:10.3390/nu10111786
- Allen NE, Key TJ. The effects of diet on circulating sex hormone levels in men. Nutr Res Rev. 2020;13:159-184. doi:10.1079/095442200108729052
- Mínguez-Alarcón L, Chavarro JE, Mendiola J, et al. Fatty acid intake in relation to reproductive hormones and testicular volume among young healthy men. Asian J Androl. 2017;19(2):184-190. doi:10.4103/1008-682X.190323
- Cangemi R, Friedmann AJ, Holloszy JO, Fontana L. Long-term effects of calorie restriction on serum sex-hormone concentrations in men. Aging Cell. 2010;9(2):236-242. doi:10.1111/j.1474-9726.2010.00553.x
- Misra M, Klibanski A. Anorexia nervosa and its associated endocrinopathy in young people. Horm Res Paediatr. 2016;85(3):147-157. doi:10.1159/000443735
- Harris MA. The relationship between physical inactivity and mental wellbeing: Findings from a gamification-based community-wide physical activity intervention. Heal Psychol Open. 2018;5(1). doi:10.1177/2055102917753853
- Viña J, Sanchis-Gomar F, Martinez-Bello V, Gomez-Cabrera MC. Exercise acts as a drug; The pharmacological benefits of exercise. Br J Pharmacol. 2012;167(1):1-12. doi:10.1111/j.1476-5381.2012.01970.x
- Ari Z, Kutlu N, Uyanik BS, Taneli F, Buyukyazi G, Tavli T. Serum testosterone, growth hormone, and insulin-like growth factor-1 levels, mental reaction time, and maximal aerobic exercise in sedentary and long-term physically trained elderly males. Int J Neurosci. 2004;114(5):623-637. doi:10.1080/00207450490430499
- Priskorn L, Jensen TK, Bang AK, et al. Is Sedentary Lifestyle Associated With Testicular Function? A Cross-Sectional Study of 1,210 Men. Am J Epidemiol. 2016;184(4):284-294. doi:10.1093/aje/kwv338
- Afrisham R, Sadegh-Nejadi S, SoliemaniFar O, et al. Salivary testosterone levels under psychological stress and its relationship with rumination and five personality traits in medical students. Psychiatry Investig. 2016;13(6):637-643. doi:10.4306/pi.2016.13.6.637
- Hallberg SJ, Gershuni VM, Athinarayanan SJ. Reversing type 2 diabetes: A narrative review of the evidence. Nutrients. 2019;11(4):1-16. doi:10.3390/nu11040766
- Wu Y, Ding Y, Tanaka Y, Zhang W. Risk factors contributing to type 2 diabetes and recent advances in the treatment and prevention. Int J Med Sci. 2014;11(11):1185-1200. doi:10.7150/ijms.10001
- Sadat-Ali, M., Al-Anii, F. M., Al-Turki, H. A., AlBadran, A. A., & AlShammari, S. M. (2018). Maintenance Dose of Vitamin D: How Much Is Enough?. Journal of bone metabolism, 25(3), 161–164. https://doi.org/10.11005/jbm.2018.25.3.161
- Saper, R. B., & Rash, R. (2009). Zinc: an essential micronutrient. American family physician, 79(9), 768–772
- Sato J, Kanazawa A, Azuma K, et al. Probiotic reduces bacterial translocation in type 2 diabetes mellitus: A randomised controlled study. Sci Rep. 2017;7(1). doi:10.1038/s41598-017-12535-9
- Tian S, Xu Q, Jiang R, Han T, Sun C, Na L. Dietary protein consumption and the risk of type 2 diabetes: A systematic review and meta-analysis of cohort studies. Nutrients. 2017;9(9):1-17. doi:10.3390/nu9090982


