Gold Standard TRT

In my professional opinion, gold standard TRT is daily subcutaneous injections of Testosterone Enanthate or Cypionate and HCG, this is something I discuss in detail in TRT Best Practice. The aim of Testosterone Replacement Therapy (TRT) is to restore your androgen levels to within normal physiological parameters. The aim of Testosterone Optimisation Therapy (TOT) is to optimise your androgen levels so that you feel the qualitative and quantitative benefits of having healthy hormonal levels. They should not be mutually exclusive, they should be the same thing. This is why we carefully titrate the prescribed dose of testosterone and HCG according to effect. TRT must be personalised as we are all biologically unique, you cannot have a one size fits all approach to hormonal health.
What Is the Purpose of TRT?
The primary role of hormones is to help maintain homeostasis, a complex process that involves biochemical and physiological mechanisms to help achieve an equilibrium or stability within the body. By that rationale, the aim of TRT and TOT is to restore your levels and achieve stability. The qualitative effects of TRT are due to stable levels with the correct androgen ratio of the different hormones.
How Is Stability Achieved?
For us to understand this, we need to understand both pharmacokinetics, which is what the body does to the testosterone once administered, and pharmacodynamics, which is what the testosterone does in the body.
Route of Administration
It comes as no secret that both subcutaneous and shallow intramuscular injections are the most effective method of delivering a consistent dose of testosterone to the bloodstream. Subcutaneous injections have two significant advantages over intramuscular injections, they are less painful and the rate of absorption is slower causing less aromatisation of testosterone to oestradiol. Whilst oestrogen is incredibly important in cognitive function, mood, libido, fertility, cardiovascular health and maintaining bone strength, too much is as bad as too little. Whilst topical application of testosterone cream or gel remains a reasonable choice of delivery method, there are potential limitations to its efficacy due to inconsistent absorption with the skin barrier.
Pharmacokinetics 1-0-1 & How it Relates to Your Choice of Testosterone Ester
There is considerable variation in the half-life of unbound testosterone, ranging from 10 to 100 minutes. Esters are attached to the testosterone molecule by a process called hydrolysis. Esters are essentially a class of organic compounds that react with water to produce alcohols and organic or inorganic acids. This equates to a chain of carbon atoms that makes the molecule less soluble. The testosterone molecule can only become bioavailable when enzymes from the liver break down the carbon chains releasing the testosterone. The longer the carbon chain, the longer this process takes.
Testosterone Cypionate
Testosterone Cypionate is our preferred choice of ester for gold standard TRT. It is also the preferred choice of ester in the USA, where Testosterone Deficiency and TRT is more commonly and widely accepted. We are the first private medical clinic in the UK to import Testosterone Cypionate in the UK for our patients. Through clinical experience, I have become a huge proponent of daily subcutaneous Testosterone Cypionate injections, not only to achieve stable male androgen levels, but also to mimic natural physiology. In some patients with high-normal Sex-Hormone Binding Globulin levels, it is possible to achieve stable levels with a less intensive injection frequency, however there is a reported qualitative difference in well-being with daily injections.
There is natural diurnal variation in testosterone levels throughout the day, with levels being at their highest in the morning as anabolic processes predominate at night. Irrespective of how stable your levels are, by the very nature of injecting a hormone, there will be a slight peak and so daily injections makes perfect sense. The similarity in ester length in both Testosterone Cypionate and Testosterone Enanthate, makes them essentially interchangeable. However, the increased fluidity of the olive oil solvent in Testosterone Cypionate, alongside its low concentration of Benzoyl Alcohol preservative, makes Cypionate a preferable choice for subcutaneous injections.
Testosterone Enanthate
Testosterone Enanthate contains the carboxylic acid ester, enanthoic acid. It has a half-life of approximately 7-9 days. According the British National Formulary, a single dose of 250mg Testosterone Enanthate should be injected every 2-3 weeks(1). According to the manufacturer, a single injection of 250mg leads to an increase in total plasma testosterone between 44.5-60.4 nmol/l (Cmax), which is reached within 0.5 – 5 days post injection. It was also noted that testosterone levels returned to baseline typically after 2 weeks, so the suggested 3-week injection frequency would be ineffective in rising baseline figures(2).
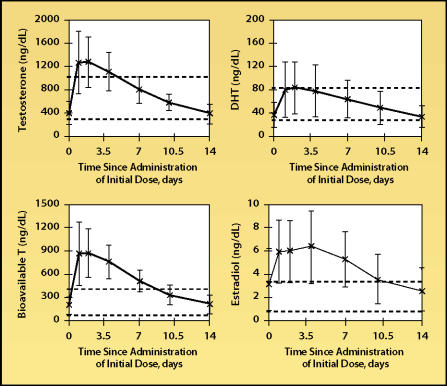
Steady-state mean serum levels of testosterone, bioavailable testosterone (T), dihydrotestosterone (DHT), and estradiol in thirty-three hypogonadal 22- to 65-year-old men given 200 mg of intramuscular testosterone enanthate every 2 weeks. Error bars indicate standard deviations. Dashed lines denote upper and lower limits of normal range. Adapted, with permission, from Dobs et al.7(3)
Sustanon
Sustanon contains a blend of four esters:
-
30mg Propionate
Half-life approximately 3.5 days
-
60mg Phenylpropionate
Half-life approximately 4.5 days
-
60mg Isocaproate
Half-life approximately 9 days
-
100mg Decanoate
Half-life approximately 15 days
The pharmacokinetic properties of Sustanon are not too dissimilar to that of Testosterone Enanthate. Sustanon has a Cmax of approximately 70nmol/l, which is reached approximately 24-48 h (tmax) after administration. Levels then return to baseline after approximately 21 days, longer than Enanthate, presumably due to the longer half-life of the decanoate ester(4). In theory, this blend of esters with varying half-life’s was designed to reduce the peaks and troughs associated with the metabolism of the testosterone. Unfortunately, in practice, this is not the case.
Nebido (Testosterone Undeconate)
Nebido contains the long undecanoic acid ester. Its half-life is approximately 90 days, with stability being achieved in approximately 450 days.
Due to the long-acting nature of this compound, a loading dose is recommended at six weeks. The Cmax 7 days after the first injection was noted to be 38 nmol/L, this rose to 50nmol/l after the 6-week loading dose was administered. Once stable, the mean Cmax was noted to be 37nmol/l and the Cmin was 16 nmol/L, with a 10-week dosing interval. The median intra- and inter-individual variability (coefficient of variation, %) of Cmin values was 22 % (range: 9-28%) and 34% (range: 25-48%), respectively(5).
Why a Cookie-Cutter Approach Doesn’t Work
It is recognised that there is variance of the peak and trough levels between individuals(6) and so the data cannot apply to everybody. We all have a unique genetic blue-print, no one person’s physiology is identical to that of another.
The primary aim of TRT is to achieve stable hormone levels within the body so that homeostasis is maintained. The above data demonstrates that the current recommendations regarding dose and injection frequency do not achieve this.
When choosing a testosterone, it’s important to understand how long it will typically take to achieve a ‘steady state’. This is when the rate of drug input is equal to the rate of drug output. Irrespective of your choice, it is impossible to achieve true stability, something I talk about in The Perfect TRT Protocol. It is recognised that it takes approximately 5 half-lives for this to occur.
Steady state according to the different esters available:
Testosterone Enanthate / Cypionate
- 35-45 days
Sustanon
- Propionate Ester – 17.5 days
- Phenylpropionate Ester – 22.5 days
- Isocaproate Ester – 45 days
- Decanoate Ester – 75 days
Nebido (Testosterone Undeconate)
- 450 days
The aim of dosing is to build up the plasma concentration of testosterone so that it achieves an optimal level according to your genetics, physiology and utilisation. You cannot predetermine that number based on the current data. The current UK reference range of 12-29 nmol/l is very non-specific, doctors do not take age into consideration despite knowing there is an age-related decline in testosterone. This is an arbitrary discussion since we know there are health benefits in having a testosterone above 19nmol/l(7).
You must first understand that the total testosterone level is not a true marker by which qualitative and quantitive symptoms can be gauged. Total testosterone is not bioavailable, it is simply the precursor to the bioavailable androgens, free testosterone, oestradiol and dihydrotestosterone. It is still important because it must be taken in context with other proteins in the body, such as Sex Hormone Binding Globulin (SHBG) which binds to testosterone preventing it from becoming bioavailable. SHBG serves an important role in helping mediate the transfer of testosterone into the cells for its primary function, cell growth and repair. There is a correlation between low testosterone and low SHBG which has implications for cardiovascular disease and increased insulin resistance(8). Another protein to be taken into consideration is albumin, formed in the liver, which has a weaker affinity for testosterone so still reduces the free testosterone level.
Testosterone is lipid soluble which means it can permeate cell membranes to enter the cell to exert its effects. It has a high volume of distribution, this information helps you calculate the dose needed to achieve a critical plasma concentration. As already mentioned, there is individual variation in drug metabolism of the different esters and there is no defined optimal testosterone level, so you cannot apply a standard fixed dose and frequency of injection to achieve stability. Therefore, to titrate your optimal dose and frequency, it is sensible to use only one variable. It also makes sense that the action of this variable should be predictable, something that has been demonstrated with testosterone enanthate; oestradiol and DHT levels exhibit saturable increases with increased dose(9).
More frequent smaller doses are often better at achieving actual steady levels. SHBG which binds to testosterone is often the determining factor in deciding injection frequency. If the injection frequency is too long, you can reach a steady state, yet that term will be a relative one and you will still notice peaks and troughs as the testosterone is metabolised and excreted by the kidneys as conjugates of glucuronic and sulfuric acids in urine at a high rate.
IMPORTANT
Gold standard TRT includes Human Chorionic Gonadotropin (HCG) alongside testosterone. I haven’t gone into detail on The Benefits of using HCG with TRT or our TRT Management Guidelines as these have been covered in previous blogs. Please click on the links for further information.
Discussion
When The Men’s Health Clinic opened in January 2016, we looked at the various treatment options available in the UK. Nebido (Testosterone Undeconate) was the UK licenced drug for the treatment of Testosterone Deficiency Syndrome. We were enthused by the product description which assured us of realistic steady levels, the absence of peaks and troughs, the need for infrequent injections and there being no direct transfer since it is administered via the intramuscular route. So a direct comparison to Sustanon and Testogel, hence the marketing.
As an aside, Sustanon is an interesting blend of esters, it was designed to achieve stable levels. I have heard a few amusing metaphors justifying the mix of esters. The Propionate ester is the ‘sprinter’, the Phenylpropoionate and Isocaproate esters are ‘middle distance runners’, and the Decanoate ester is a ‘long distance runner’, with each respective ester taking over the baton to keep a constant pace. I mean honestly! Perhaps it made sense after a few glasses of scotch! In practice, it appears that the shortest acting ester, Propionate, is the most important determinant in deciding the optimal protocol for relative stability. So with a normal SHBG, I would recommend every other day injections. However, the high Benzoyl Alcohol content of Sustanon which can cause post injection pain (PIP) makes that a rather unappealing proposition. Sustanon is prescribed because it’s cheap, dirt cheap, sometimes you just get what you pay for. It is difficult to achieve stable levels on Sustanon and providers often resort to an aromatase inhibitor or ‘third leg of TRT’ to reduce oestrogen. I don’t use Sustanon, only the best for my patients!
We opted for Nebido and followed the treatment guidelines, administering a loading dose at six weeks with subsequent follow up bloods twelve weeks later. The vast majority of men had numbers not too dissimilar to pre-treatment levels, along with pituitary suppression of Lutenising Hormone (LH) and Follicle Stimulating Hormone (FSH), something that is expected on TRT. There were a few outliers who had residual pituitary function, these patients were noted to have a primary hypogonadism, their total testosterone levels were still only just above baseline.
Patients using Nebido did report an initial qualitative improvement in their symptoms, however as the weeks went on they noticed a dip or trough, with a return of their symptoms of low testosterone. This essentially negated the argument for a loading dose with the next injection interval being twelve weeks. In response, we decreased the interval between the loading dose and the 3rd dose to ten weeks for new patients. Despite this, patients were still complaining of peaks and troughs. Injection intervals were shortened further over time for our regular patients until reasonable trough levels were achieved. Unfortunately, this raised a further set of problems. As already discussed, the aim of TRT and TOT is to achieve sustainable stable levels that bring about, not only the correct total testosterone level, but also optimal levels of the bioavailable markers; free testosterone, oestradiol and dihydrotestosterone. Shortening the interval between injections brought about sustained symptoms of supraphysiological markers of excess free testosterone, oestradiol and dihydrotestosterone. The temporary issue of a few weeks of some breast tissue swelling, nipple tenderness, water retention and acne was bad enough, but to have sustained symptoms was intolerable.
In view of our experiences with Nebido, we looked to the American model for managing TDS. They were using short-acting esters, such as enanthate and cypionate (both are interchangeable), and were achieving stable levels that were backed up with a noted improvement in their symptoms. Their model was far more progressive, they were not only managing total testosterone, they were also monitoring and managing high oestradiol and dihydrotestosterone. They also considered the benefits of using HCG alongside TRT.
We have had great success in achieving not only sustainable stable levels with the use of testosterone enanthate/cypionate, but also the subjective and objective qualitative and quantitative changes that each patient has sought from TRT. Whilst the majority of our patients are on Testosterone Cypionate as this is our gold standard, some of my patients are fortunate enough to have their testosterone prescribed through the NHS, under my guidance and supervision. Disappointingly, Testosterone Cypionate is not available through the NHS. Have a read of the testimonials page of our website to see the positive impact that gold standard TRT, clinical input and care has had on our patients.
Conclusion
Achieving stable levels is all about tailoring injection dose and frequency according to need, and titrating that level up or down according to both qualitative and quantitve markers. I hope it’s now clear why I use Testosterone Cypionate (or Enanthate if prescribed via the NHS) as my gold standard TRT at The Men’s Health Clinic. You cannot have a cookie-cutter approach to TRT. Keep it simple, keep it safe.
Dr Robert Stevens MBChB MRCGP Dip.FIPT


